







 June 4, 2024
June 4, 2024Forty-six percent of transgender and non-binary youth in the United States have seriously considered suicide, and among those individuals, thirty percent have attempted it. This harrowing reality is brought to light in a study conducted by the Trevor Project, a non-profit organization focused on suicide prevention of queer youth. Their study shows that gender nonconformity is not a trend but a matter that needs to be addressed, and that it must be done so with urgency and care. Meanwhile, on April 29th, 2023, theoretical physicist Sabine Hossenfelder released a YouTube video titled, “Is being trans a social fad among teenagers?”. Between faulty and misconstrued information, Hossenfelder’s attempt to help people understand transgenderism falls short of what should be viewed as competent. The video is misleading due to reliance upon faulty information and use of the false balance fallacy. In order to maintain trust with the widest possible audience, she paints a narrative that portrays herself as a neutral party against two equally radical extremes, which is to the expense of her data’s accuracy.
Sabine Hossenfelder
Before examining the claims she makes, it is important to understand Sabine Hossenfelder and how she frames herself within the matter of gender dysphoria in adolescents. “[T]here are normal people, like you and I, who think both sides are crazy and [would like someone to] summarize the facts in simple words, which is what I’m here for” (0:25). Sabine Hossenfelder is a theoretical physicist who specializes in quantum gravity. She has a PhD in theoretical physics and a bachelor’s degree in mathematics. She is known for her research within a variety of topics relating to physics, with two books and over eighty research papers in various areas of the field. In addition, she is the creative director of her eponymous YouTube channel on which she, according to her personal website, “talks about recent scientific developments and debunks hype”.
Hossenfelder has no certifications in any areas of psychology, gender dysphoria, or the use of gender-affirming care, not in adolescents nor otherwise. Her YouTube channel is used as a means of providing funding to her research in the field of physics. In an article written by journalist Margherita Cole, the for-profit nature of Hossenfelder’s YouTube career is discussed. Cole states that “she uses her thousands and sometimes millions of views to fund her research in quantum gravity. She even has sponsors and receives donations from Patreon, which add to her income”. Within her videos, Hossenfelder portrays herself as a mediator in a field that is muddled with absurdities from both sides. While oftentimes she presents correct information, it may not be evaluated for its true worth. Provably false information is also presented at times and is given more merit than it is deserving of.
Puberty blockers and hormone therapy are effective in providing benefit to adolescents
Hossenfelder falsely discredits the effectiveness of puberty blockers and hormone therapy used in adolescents. “Evidence that […] children would benefit from puberty blockers or hormone therapy is slim” (24:10). She cites a study titled Mental Health Outcomes in Transgender and Nonbinary Youths Receiving Gender-Affirming Care, showing skepticism due to its small sample size but acknowledging an existing trend, reiterating that “the mental health of those who were not treated got worse” (21:27).
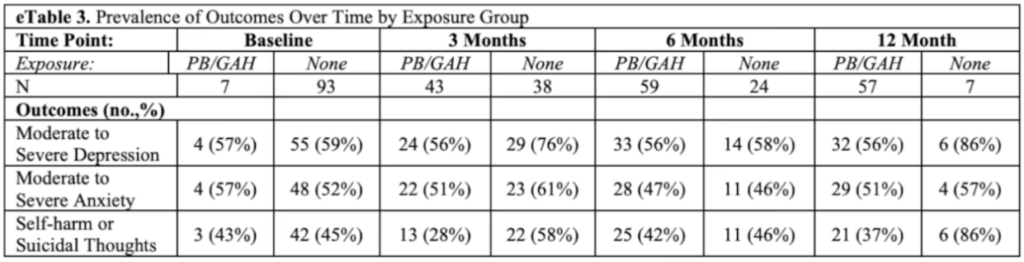
Fig. 1. The data from a study disputed by Hossenfelder for its small control group by the time of the twelfth month
The conclusion made by Hossenfelder seems to entirely disregard the wide variety of studies which have affirmed the improvements given with puberty blockers and hormone therapy in adolescents. For instance, an article written by a group of psychologists for the Journal of Sexual Medicine reports that after use of pubertal suppressants, “[b]ehavioral and emotional problems and depressive symptoms decreased, while general functioning improved significantly during puberty suppression”. Another study titled Association of Gender-Affirming Hormone Therapy With Depression, Thoughts of Suicide, and Attempted Suicide Among Transgender and Nonbinary Youth was conducted by researchers of the Trevor Project. The study demonstrates that “[u]se of [gender-affirming hormone therapy, or GAHT] was associated with lower odds of recent depression […] and seriously considering suicide […] compared to those who wanted GAHT but did not receive it”. Furthermore, the confusion of Hossenfelder surrounding the results in the study of puberty blockers stems from a misunderstanding of their purpose. The Mayo Clinic states that puberty blockers “pause puberty [to offer] a chance to explore gender identity”. Placing a pause on puberty will slow the progression of the gender dysphoria caused by it and therefore will allow one to maintain their mental health, whereas being without it when it is necessary will create a decline in mental health. Additionally, Hossenfelder misrepresents the credibility of the study she had cited under the argument that it is of too low of a sample size for consideration. However, the samples between three and six months contain thirty-eight and twenty-four individuals within their respective month of those who have not underground gender-affirming care. The number of those individuals at the six month point is over three times that of the twelve month point, and the data collected demonstrates “that depressive symptoms and suicidality were 2-fold to 3-fold higher than baseline levels at 3 and 6 months of follow-up, respectively” (see fig. 1). The study should be acknowledged for its observable trends in the time where its control group is considerable. Altogether, these studies further undermine Hossenfelder’s claim that puberty blockers and hormone therapy result in minimal improvements.
Rapid Onset of Gender Dysphoria is a discredited hypothesis and is not of use in understanding transgenderism
Hossenfelder gives excessive exposure to the controversial study of Rapid Onset of Gender Dysphoria, which may lead the uninitiated viewer astray. “[A]t the moment, there is no conclusive evidence neither for nor against the existence of rapid onset gender dysphoria, though it seems to be supported by anecdotal reports from doctors working in clinics who treat the children” (10:42). Hossenfelder spends a considerable amount of time discussing the theory of Rapid Onset of Gender Dysphoria, or ROGD, an acronym coined by and often associated with Lisa Littman. Within the initial publication of her research of the theory’s validity, Littman hypothesizes that ROGD may be caused by “social influences and maladaptive coping mechanisms”. The hypothesis is controversial among researchers due to the methods Littman used in the collection of data in her studies and the theory’s lack of proven basis outside of that data. A research article written by Florence Ashley of PsychCentral highlights significant bias within the study, stating that “[t]he study was based on the reports of parents recruited from well-known, anti-trans websites”. SpringerLink, one academic database that hosted the study, ultimately retracted it “due to noncompliance with [their] editorial policies around consent”, further demonstrating the unprofessional nature of the study.
ROGD is presented as an important talking point by Hossenfelder when in reality, it is only a hypothesis, one which is highly discredited. The World Professional Association for Transgender Health, or WPATH, regards the concept as “nothing more than an acronym created to describe a proposed clinical phenomenon that may or may not warrant further peer-reviewed scientific investigation”. In an interview with Scientific American, the president of WPATH, Marci Bowers, evaluates ROGD as “a fear-based concept that is not supported by studies” that intends to “scare people or to scare legislators into voting for […] restrictive policies that take away options for young people”. When making a video for individuals with little to no knowledge of the subject matter, it is misleading to cite such a theory as notable in considering a phenomenon such as gender dysphoria. Moreover, her claim of anecdotal reports by qualified doctors endorsing the theory is not expanded upon beyond this passing claim and it is difficult to verify whether the claim has any basis due to her lack of corroboration. In making this claim without a basis, she relies on the uninformed viewer entirely placing their faith in her trustworthiness. She further strengthens her false balance rhetoric by portraying rapid onset of gender dysphoria as a study of ambiguous validity while also skewing it slightly in its favor.
Puberty blockers do not necessarily cause long-term impacts on bone density
Hossenfelder makes claims about puberty blockers that are ignorant of decades of past research. “There are few long-term studies on people who have been taking puberty blockers, but those that exist show that bone density is unlikely to entirely recover, which means a life-long increase of the risk to break bones” (14:35). This claim stems from the changes to bone mineral density that are prevalent after use of gonadotropin-releasing hormone analogs, or GnRHa, a type of puberty blocker. GnRHa is a type of treatment also used in those with central precocious puberty, or CPP, where one experiences an onset of puberty sooner than they are meant to. Some additional research surrounding the relation between GnRHa and CPP suggests associations to bone mineral density, or BMD. A study focused on GnRHa published in the 151st volume of the European Journal of Endocrinology states that GnRHa “may theoretically have a detrimental effect on bone mass during pubertal development”.
While some research is still being conducted within the area, available studies show that long-term impacts on bone density caused by use of GnRHa in transgender adolescents does not seem to last long-term. A study by a group of scientists published on Karger titled Use of Gonadotropin-Releasing Hormone Analogs in Children: Update by an International Consortium considers the use of GnRHa in relation to transgender individuals. Within their research, they conclude: “GnRHa treatment slows mineral accrual, but after discontinuation BMD appears not to be significantly different from that of their peers by late adolescence”. Hormone blockers are generally used for only a few years before one would begin hormone replacement therapy. The concern is often in the use of hormone blockers for longer periods of time, which typically will not happen among transgender individuals. Hossenfelder’s claim that the area of puberty blockers is one that is underdeveloped is false. An article written by a group of pediatricians in the National Center for Biotechnology Information concurs: “Since 1981, GnRHa administration has been the standard treatment for CPP”. Studies surrounding the existence of GnRHa have been around for decades, and so the scientific background is there so that we can draw such conclusions safely.
Assigned gender at birth is not closely correlated with transgenderism
Hossenfelder makes misleading claims surrounding the proportion of the assigned birth gender of transgender individuals. “Curiously enough, the big bulk of the increase comes from children assigned female at birth, wishing to transition to male” (7:59). She declares that “[t]he same thing has been observed in the Netherlands, in Spain, the UK, Canada, Sweden, and is also the case in the USA” (8:15). The study she cites and uses visual aid of is titled Re-evaluation of the Dutch approach: are recently referred transgender youth different compared to earlier referrals? and contains data of participants from “1072 persons included in this study [who] were all consecutively referred adolescents […] who registered at the Center of Expertise on Gender Dysphoria in Amsterdam, The Netherlands”. This study should not be used to indicate a ratio of the assigned birth sexes of transgender individuals anywhere outside of the Netherlands, as there is no evidence that this is a consistent trend between countries.
As a United States-centric paper, the country whose ratio of assigned birth sexes of transgender people will be analyzed is the US. Conducted by a group of psychiatrists and published by the American Academy of Pediatrics, the study Sex Assigned at Birth Ratio Among Transgender and Gender Diverse Adolescents in the United States aims to view the relation between assigned sex at birth and tendencies of transgenderism. After organizing two surveys with over two hundred thousand total participants, their findings demonstrated “an AMAB:AFAB ratio of 1.5:1 [in their 2017 survey and] an AMAB:AFAB ratio of 1.2:1 [in their 2019 survey]”. The term AMAB refers to those assigned male at birth while the term AFAB pertains to those assigned female at birth. These metrics result in the conclusion that “[t]he sex assigned at birth ratio of [transgender and gender diverse, or TGD] adolescents in the United States does not appear to favor AFAB adolescents”. The study’s findings help in understanding that while there may be different ratios of assigned birth genders between countries, there is no observable correlation between assigned gender at birth and a desire to be transgender.
Conclusion
Transgenderism is a very nuanced subject that requires careful consideration. The subject matter is being legally debated upon across the United States, making it an especially important subject to be providing proper information surrounding. Many of the claims made throughout Sabine Hossenfelder’s video demonstrate her as an unsuitable candidate for doing so. The narrative that she paints with her as an intermediary between two sides that both hold fringe beliefs is evidently false and only causes more disarray. Her misleading representations of research and use of the false balance bias help us to understand that she is far from a professional in this field and is simply looking to use it to boost her reputation and make money. This overview of Hossenfelder’s video undoubtedly shows why non-professionals shouldn’t dive head first into other lines of work.
 Prev Post
Prev Post
What do you think?
Show comments / Leave a comment